2. 10. AML guidelines: 1. I/we her eb y confirm that all pr emiums have been/will be paid fr om bonafide sour ces and no pr emiums have been/will be paid out of pr oceeds of crime r elated to any of the offence listed in pr e vention of Mone y Laundering Act, 2002. 2. I understand that the Company has the right to call for documents to establish sour ces of funds. 3. The insur ance company has right to cancel the insur ance contr act in case I am/have been found guilty b y any competent court of law under any of the statutes, dir ectly or indir ectly go verning the pr e vention of mone y laundering in India. Nationality: Indian Non – Indian If Non-Indian, please specify Country: _____________________________________________ T ype of Or ganization making the payment (Pls tick) Limited Company Go vernment Or ganization Non-Go vernmental Or ganization (NGO) Society T rust Partnership International Or ganization Cooper atives Section 25 Company Date: _________________________________ Signatur e of the Pr oposer: ___________________________________________ 7. P A YMENT DET AILS Name of the Pr emium Payer : Relationship with the pr oposer : Pr emium Amount (in Rs.) Instrument type : Cash Cheque Debit Car d Cr edit Car d Others _________ Sour ces of funds : Salary Business Others __________ Please mak e a Cr ossed Cheque/DD/Pay Or der in favour of ‘ T ata AIG Gener al Insur ance Company Limited’ only . Name of the Account Holder: Name of the Bank: T ype of Account: SB Account Curr ent Account Others (please specify) ________________________________________ Account Number : IFSC Code of Bank: If the pr emium cheque is not paid fr om the abo ve mentioned account then a cancelled cheque leaf of the abo ve mentioned account is to be attached. #mandatory if annualized pr emium is mor e than Rs.10,000 As per the Regulatory r equir ements, we can effect payment of r efund / claims only thr ough Electr onic Clearing System (ECS) / National Electr onic Funds T r ansfer (NEFT) / Real Time Gr oss Settlement (RT GS) / Interbank Mobile Payment Service (IMPS). For this purpose please submit the follo wing details of the insur ed' s bank account# Bank Details 8. A GENT DECLARA TION I,_________________________________________________________________ (Full Name) in my capacity as an Insur ance Advisor/ Specified Person of the Corpor ate Agent/Authorized emplo yee of the Br ok er/Relationship Officer, do her eb y declar e that I have e xplained all the contents of this Pr oposal Form, including the natur e of the questions contained in this Pr oposal Form to the Pr oposer including statement(s), information and r esponse(s) submitted b y him/her in this Pr oposal Form to questions contained her ein or any details sought her ein will form the basis of the Contr act of Insur ance between the Company and the Pr oposer, if this Pr oposal is accepted b y the Company for issuance of the Policy . I have further e xplained that if any untrue statement(s)/ information/r esponse(s) is/ar e contained in this Pr oposal Form/including addendum(s), affidavits, statements, submissions, furnished/to be furnished, the Company shall have the right to vary the benefits which may be payable and further mor e if ther e has been a non-disclosur e of any material fact, the policy issued to his/her favor pursuant to this Pr oposal may be tr eated b y the Company as null and void and all pr emiums paid under the Policy may be forfeited to the company . License No.(Intermediary/Corpor ate Agent/Br ok er/Relationship Officer) Name of the specified Person and code Place: __________________________ Date: __________________________ Signatur e of Agent: __________________________ 9. V ernacular Declar ation (Certification in case the pr oposer has signed in vernacular/thumb print) The content of this form along with pr oduct benefits, terms/conditions and e x clusions have been clearly e xplained b y me in vernacular to the pr oposer who has understood and confirmed the same. Signatur e/Thumb impr ession of the Pr oposer: ____________________________________________________ ____________________________________________________ Name & Signatur e of agent/intermediary: ____________________________________________________ ____________________________________________________ 11. DECLARA TION & W ARRANTY ON BEHALF OF ALL PERSONS PROPOSED T O BE INSURED l I her eb y declar e, on my behalf and on behalf of all persons pr oposed to be insur ed, that the abo ve statements, answers and/or particulars given b y me ar e true and complete in all r espects to the best of my kno wledge and that I am authorized to pr opose on behalf of these other persons. l I understand that the information pr o vided b y me will form the basis of the insur ance policy , is subject to the Boar d appr o ved underwriting policy of the insur er and that the policy will come into for ce only after full payment of the pr emium char geable. l I further declar e that I will notify in writing any change occurring in the occupation or gener al health of the life to be insur ed/pr oposer after the pr oposal has been submitted but befor e communication of the risk acceptance b y the company . l I d e c l a r e t h a t I c o n s e n t t o t h e c o m p a n y s e e k i n g m e d i c a l i n f o r m a t i o n f r o m a n y d o c t o r o r h o s p i t a l w h o / w h i c h a t a n y t i m e h a s a t t e n d e d o n t h e p e r s o n t o b e i n s u r e d / p r o p o s e r o r f r o m a n y p a s t o r p r e s e n t e m p l o y e r c o n c e r n i n g a n y t h i n g w h i c h a ff e c t s t h e p h y s i c a l o r m e n t a l h e a l t h o f t h e p e r s o n t o b e i n s u r e d / p r o p o s e r a n d s e e k i n g i n f o r m a t i o n f r o m a n y i n s u r e r t o w h o m a n a p p l i c a t i o n f o r i n s u r a n c e o n t h e p e r s o n t o b e i n s u r e d / p r o p o s e r h a s b e e n m a d e f o r t h e p u r p o s e o f u n d e r w r i t i n g t h e p r o p o s a l a n d / o r c l a i m s e t t l e m e n t . l I authorize the company to shar e information pertaining to my pr oposal including the medical r ecor ds of the insur ed/pr oposer for the sole purpose of underwriting the pr oposal and/or claims settlement and with any Go vernmental and/or Regulatory authority . l I have understood the purpose of Aadhar authentication and her eb y state that I have no objection in pr o viding my Aadhar details. l I her eb y declar e that I am a Salaried / Self Emplo yed person & my Gr oss Annual Income is (Rs ‘000) : Rs __________________________________________________________ I understand that the Sum Insur ed opted for will not be gr eater than 10 times / 20 times Gr oss Annual Income as per belo w: In case of Salaried Person – Max 10 times of Income (as appearing in Form 16/ Salary Slip/ IT ackno wledgement) l In case of Self – Emplo yed Person – Max 20 times of Income (as appearing in IT ackno wledgement / Audited P&L) l GoGr een: I would lik e to pr otect my envir onment and would lik e to help save paper b y authorizing T ata AIG Gener al Insur ance Company Limited to send all my policy and service r elated communication to the email id as mentioned in this application form. 12. FOR OFFICE USE ONL Y T ata AIG Office Code : _____________________________________________________________ Intermediary Code and Name: _______________________________________________________ Br anch Receipt Date: _____________________________________________________________ Channel T ype: _______________________________________________________________________ Business T ype: Urban/ Rur al/ Social : ______________________________________________ Customer ID : ________________________________________________________________________ Disclaimer: Insur ance is the subject matter of solicitation. For mor e details on benefits, e x clusions, limitations, terms and conditions, please r efer sales br ochur e / policy wor dings car efully , befor e concluding a sale. A CKNO WLEDGEMENT (T O BE GIVEN T O CUST OMER) Application Number: _______________________ Date: ______________________ Name of the Pr oposer _________________________________________________________________________________ W e ackno wledge with thanks the r eceipt of your application for Accident Guar d Plus and amount b y cash/cheque/Demand Dr aft/others _______________________________________________ of amount of Rs.___________________________________. Neither the submission to us of a completed pr oposal for insur ance nor any payment to war ds this application obliges us to agr ee to issue a policy , which decision is and always shall be in our sole and absolute discr etion. If we accept a pr oposal for insur ance, it shall be subject to the policy terms and conditions and we shall have no liability to mak e any payment if pr oposal is not accepted b y us or pr emium is not r eceived b y us in full and in time and/or non-fulfillments of additional information r equested b y us. W e shall have no liability to mak e any payment under the Policy if pr oposal is under-pr ocess & claim arises in the interim period befor e the decision on the pr oposal is given b y us. If we do not accept the pr oposal, we will inform you and r efund any payment r eceived fr om you without inter est within ne xt 15 days fr om the date of underwriting decision on the pr oposal. T oll Fr ee No. (24x7): 1800 266 7780 or 1800 229966 (For Senior Citizens) W ebsite: UIN: T A TP AIP18044V011819
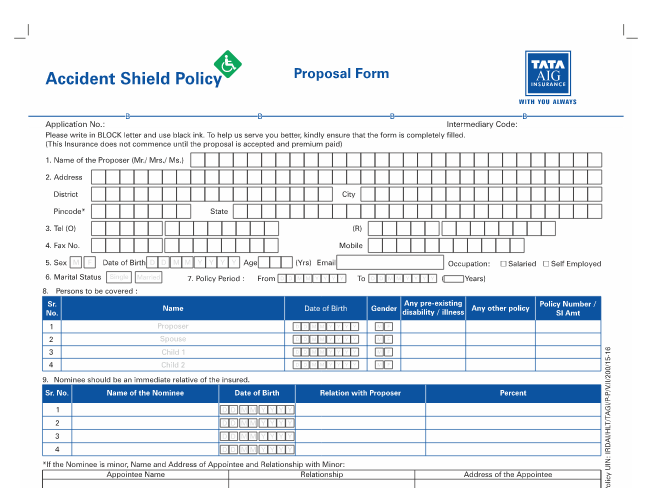
1. 3. DET AILS OF THE PERSON(S) T O BE INSURED Sl. Name of the Gender Relationship with DOB Aadhaar No. Risk Monthly No. Insur ed Person Pr oposer* Class** Income 1. M / F DD/MM/YYYY 2. M / F DD/MM/YYYY 3. M / F DD/MM/YYYY 4. M / F DD/MM/YYYY 5. M / F DD/MM/YYYY * A l l o w e d r e l a t i o n s – S p o u s e , c h i l d r e n a n d emplo yee ** Risk Class as per natur e of duties to be selected # (Mandatory in case of pr emium > Rs.1 Lac) (In case pr oposer is not an individual entity then d e t a i l s o f t h e e n t i t y t o b e f i l l e d , PA N i s mandatory for such cases) • Sum Insur ed available in Units of 5 Lakhs, upto 5 Cr or es (multiples of 5 Lacs) • Spouse eligible for 50% of the primary insur ed member ’ s Sum Insur ed • Childr en eligible for 10% of the primary insur ed member ’ s Sum Insur ed 1. This is an application for insur ance and issuance of this does not amount to acceptance of pr oposal b y us. Commencement of risk under this pr oposal is subject to acceptance of the risk b y us and r eceipt of pr emium. 2. The information declar ed b y you in this form is the basis for issuance of the policy . 3. Please answer all questions car efully . Any incomplete, incorr ect or partially corr ect answers may lead to r ejection of the pr oposal and also might lead to cancelation of policy . Please fill-up this form in CAPIT AL LET TERS 4. NOMINEE DET AILS In the e vent of the death of the Pr oposer any payment due under the Policy shall become payable to the nominee in accor dance with the Policy terms and conditions. The nominee must be an immediate r elative of the Pr oposer. Nominee / Assignee DOB Relationship Addr ess % RISK CLASS** • Occupation Class I - Individuals in non-hazar dous occupations with office or tr avel duties, such as e x ecutives, senior management of companies with administr ative functions, bank ers, accountants, lawyers, and similar occupations. • Occupation Class II – Individuals facing limited e xposur e to occupational hazar ds with superintending, engineering or medical duties, such as plant superintendents, engineers, physicians, inspectors and similar occupations. • Occupation Class III - Individuals with occupational hazar ds, such as industrial work ers, most of whom ar e skilled or semi-skilled work ers using machinery . Also in this gr oup will be found filling station attendants, farmers, tr adesmen and delivery clerks. • Occupation Class IV - Individuals with occupational hazar ds, such as industrial work ers using heavy machinery or unskilled labor ers. • Occupation Class V – members who ar e not engaged in any occupation for livelihood including r etir ed members, non-earning childr en, house wives, dependent par ents etc • If a member has mor e than one occupation (eg: farmer who o wns a r etail shop) the higher of the two occupation classes would be consider ed for r ating. 5. ANY O THER PERSONAL A C CIDENT POLICY DET AILS Is the pr oposer or any of the persons pr oposed, alr eady Insur ed under a personal accident plan with T ata AIG Gener al Insur ance Company Ltd. or any other insur er or is a pr oposal pending for Policy issuance? If yes, please indicate the Policy/ Application number(s): ________________________________________ Policy No. Name of Insur ed Person Insur er Sum Insur ed (Rs) Claims lodged during the pr eceding years 1 2 3 4 5 6 7 Y / N Y / N Y / N Y / N Y / N Y / N Y / N Please answer each of the follo wing questions individually for each Insur ed Person b y ticking the r ele vant bo x. History of any illness/disease/injury/disability in the past other than for childbirth, flu or for URN No. AH/2017-18/P A-01minor injuries that have completely healed? 6. MEDICAL AND DISABILITY DET AILS (Medical History) : Please answer the belo w mentioned questions individually in Y es (Y) / No (N): Y ou must answer the questions truthfully . Not doing so would lead to termination of your policy . Insur ed Person * I f t h e N o m i n e e i s m i n o r , N a m e a n d A d d re s s o f A p p o i n t e e a n d Relationship with Minor: Appointee Name Relationship Addr ess Application No. ______________________ DD/MM/YYYY V ARIANT: RIDER: PRO TECT T empor ary T otal Disability (only in Pr otect variant) 2. PLAN DET AILS Pr oposed Policy Period T O Policy T enur e 1 Y ear 2 Y ear (5% pr emium discount) 3 Y ear (10% pr emium discount) Sum Insur ed (Rs.) ELITE PREMIER Loan Shield No. of childr en D D M M Y Y Y Y D D M M Y Y Y Y Child T uition Benefit (Only in Elite & Pr emier V ariant) PROPOSAL FORM Mobile No. Income (Annual) Gender: Name (Mr /Mrs /Ms /Dr) 1. PROPOSER’S DET AILS F i r s t N a m e M i d d l e N a m e S u r n a m e Addr ess City/T o wn D i s t r i c t E-Mail ID Pin Code State Ar ea Male Female Occupation: Aadhar No.: Salaried Self-Emplo yed Marital Status: Married Single Others P AN CARD No.# T ata Emplo yee Affinity Emplo yee ID No. ___________________________ Pr ohibition of Rebates - Section 41 of the Insur ance Act, 1938 as amended b y Insur ance Laws (Amendment) Act, 2015 1. No person shall allo w or offer to allo w either dir ectly or indir ectly as an inducement to any person to tak e out or r ene w or continue an insur ance in r espect of any kind of risk r elating to lives or pr operty in India, any r ebate of the whole or part of the commission payable or any r ebate of pr emium sho wn on the policy , nor shall any person taking out or r ene wing or continuing a policy accept any r ebate, e x cept such r ebate as may be allo wed in accor dance with the published pr ospectus or tables of the insur er. 2. Any person making default in complying with the pr o visions of this section shall be liable for penalty which may e xtend to ten lakh rupees. Section 64 VB of the Insur ance Act 1938 : Commencement of risk co ver under the policy is subject to r eceipt of pr emium b y T ata AIG Gener al Insur ance Company Limited. D D M M Y Y Y Y DOB: