1. Accidents ar e uncertain but Pr otection is guaranteed PERSON AL ACCIDENT IP A - 4 For internal reference only
2. All Pr emiums ar e excluding GST *T axes will be applica ble AGE BAND HOSPIT AL CASH ACCIDENT ONL Y HOSPIT AL CASH ACCIDENT AND SICKNESS 1000 per day - max upto 30 day 18 to 40 41 to 50 51 to 60 61 to 65 66 to 80 375 375 375 375 375 1080 1773 3092 5296 9000 2,769 15,00,000 15,00,000 10,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 50,000 75,000 1,00,000 3,370 25,00,000 25,00,000 10,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 50,000 1,25,000 1,00,000 3,070 20,00,000 20,00,000 10,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 50,000 1,00,000 1,00,000 8,196 75,00,000 75,00,000 15,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 50,000 3,75,000 1,00,000 5,522 50,00,000 50,00,000 15,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 50,000 2,50,000 1,00,000 17,990 1,50,00,000 1,50,00,000 30,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 1,00,000 7,50,000 1,00,000 10,721 1,00,00,000 1,00,00,000 20,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 1,00,000 5,00,000 1,00,000 29,463 2,50,00,000 2,50,00,000 50,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 1,00,000 12,50,000 1,00,000 23,726 2,00,00,000 2,00,00,000 40,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 1,00,000 10,00,000 1,00,000 1,645 10,00,000 10,00,000 10,000 1,00,000 2,000 2,00,000 10,000 50,000 20,000 50,000 50,000 1,00,000 Ad d-on Pr emium Self Plan Accidental Dea th P ermanent Disa bility (PTD+PPD) T emporar y T otal Disa bility (Upto 104 weeks) Accidental Hospitaliza tion Ambulance Charges Dependent Child Educa tion Benefit Last Rites Cost - Accident onl y Coma tose Benefit - Accident Onl y Medical Insurance Indemnity Pr emium Par ental Car e Benefit Assault Br ok en Bones (Pr emium Payable Y early) SUM INSURED 10 L AKH 15 L AKH 20 L AKH 25 L AKH 50 L AKH 75 L AKH 1 CR ORE 1.5 CR ORE 2 CR ORE 2.5 CR ORE Accidents ar e uncertain and can af fect y our f amil y's sa vings and financial planning . HDFC ERGO P er sonal Accident Insurance r eassur es y our f amil y of the ad ded pr otection and financial security tha t the y r equir e a t such a cr ucial time. FEA TURES *T er ms and Conditions apply ADDITION AL FEA TURES Coverage a vaila ble fr om ` 10 Lakhs to ` 2.5 Cr or es Optional benefit of Hospital Cash Accident Onl y & Hospital Cash Accident and Sickness Cumula ti ve Bon us of 5% incr ease in Sum Insur ed on r ene wals P olicies can be issued upto 2 y ear s Life Long Rene wa bility Age Criteria - 18 y ear s to 80 y ear s ` ` ` 5% Accidental Dea th P ermanent Disa bility (PTD+PPD) T emporar y T otal Disa bility (Up to 104 weeks) Accidental Hospitaliza tion Ambulance Charges Dependent Child Educa tion Benefit Last Rites Cost - Accident onl y Coma tose Benefit - Accident Onl y Medical Insurance Indemnity Pr emium Par ental Car e Benefit Assault Br ok en Bones ` A PREMIUM DET AIL S All f igur es in ` Printing Code:IP A4/BPF/144/OCT19
4. HDFC ERGO General Insurance Company Limited. IRD AI Re g . No . 146. CIN: U66030MH2007PL C177117. Re gister ed & Cor pora te Of fice: 1st Floor , HDFC House, 165-166 Backba y Reclama tion, H. T . Par ekh Marg , Chur chg a te, Mumbai – 400 020. Customer Ser vice Ad dr ess: D-301, 3r d Floor , Eastern Business District (Magnet Mall), LBS Marg , Bhandup (W est), Mumbai - 400 078. Customer Ser vice No: 022 - 6234 6234 / 0120 - 6234 6234 | car e@hdfcerg o .com | www .hdfcerg o .com. F or mor e details on the risk f actor s, terms and conditions, please r ead the polic y document car efull y bef or e concluding a sale. T rade Log o displa y ed a bove belongs to HDFC Ltd and ERGO Interna tional AG and used by the Company under license. UIN: P er sonal Accident Insurance - IRD A/NL-HL T/HDFC-ERGOGI/P-H/V .I/257/13-14. UID No . 3269. hdfcerg o .com 1800 2666 400 HDFC ER GO Mobile App HDFC ER GO General Insurance Compan y Limited Printing Code:IP A4/BPF/144/OCT19 PREVIOUS/CURRENT INSURANCE DET AILS If Y es, please provide the details: Is the proposer or the person(s) proposed to be insured currently insured or have been insured in the past under a Life / Accident Insurance Policy? Sr . No. 1. 2. 3. 4. 5. 6. Insurer Policy No. From Date T o Date Sum Insured Claim Details No. of Claims Amount Ailment % Amount ( ` ) Cumulative Bonus Earned Y es No (Please provide the details of premium payment)) PREMIUM P A YMENT DET AILS Premium Amount: ` Payment Option: # Cash Cheque DD Credit / Debit Card Amount in words: # Premium in Cash will be accepted only at our branch of fices. For Cheque / DD (Payable in favour of “HDFC ERGO General Insurance Company Limited”) _____________________________________________________________________________________________ D D M M Y Y Y Y Instrument Date: Instrument Amount: ` _________________________________________________________ ________ Card T ype: Name on Card: Master V isa AMEX DECLARA TION l/W e further declare that l/we will notify in writing any change occurring in the occupation or general health of the life to be insured/proposer after the proposal has been submitted but before communication of the risk acceptance by the company . l/W e declare and consent to the company seeking medical information from any doctor or from a hospital who at anytime has attended on the life to be insured/proposer or from any past or present employer concerning anything which af fects the physical or mental health of the life to be insured/proposer and seeking information from any insurance company to which an application for insurance on the life to be insured/proposer has been made for the purpose of underwriting the proposal and/or claim settlement. l/W e hereby declare, on my behalf and on behalf of all persons proposed to be insured, that the above statements, answer and/or particulars given by me are true and complete in all respects to the best of my knowledge and that l/W e am/are authorized to propose on behalf of these other persons. I understand that the information provided by me will form the basis of the Insurance Policy , is subject to the Board approved underwriting policy of the HDFC ERGO General Insurance Company Limited and that the policy will come into force only after full receipt of the premium chargeable. I/W e authorize the company to share information pertaining to my proposal including the medical records for the sole purpose of proposal underwriting and/or claims settlement and with any Governmental and/or Regulatory authority . Signature of Proposer PROHIBITION OF REBA TES - Under Section 41 of The Insurance Laws (Amendment) Act, 2015 No person shall allow or of fer to allow either directly or indirectly as inducement to any person to take out renew or continue an insurance in respect of any kind of risk relating to lives or property in India any rebate of the whole or part of the commission payable or any rebate of the premium shown on the Policy , nor shall any person taking out or renewing or continuing a Policy accept any rebate except such rebate as may be allowed in accordance with the published prospectuses or tables of the Insurer . Any person making default in complying with the provision of this section shall be punishable with fine which may extend to ` 10 Lakhs. Date : _________________________ T ime : ____________________________ SOURCES OF FUND Instrument No.: Bank Name D D M M Y Y Y Y For Credit Card / Debit Card (Only Proposer's Card to be accepted) Card No.: Expiry Date: Salary Business Other (Please Specify) _____________________________________________________________________________________________
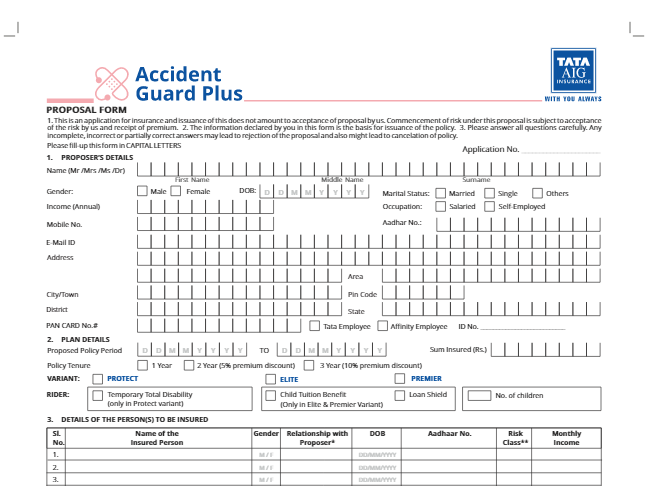
3. HDFC ERGO General Insurance Company Limited PERSONAL ACCIDENT INSURANCE - PROPOSAL FORM Please fill the form in BLOCK LETTERS. All details with* are mandatory . PLEASE USE ONL Y ORIGINAL PROPOSAL FORM. PHOT O COPIES WILL NOT BE ACCEPTED BY THE COMP ANY PROPOSER DET AILS Name*: (First Name) (Middle Name) (Last Name) Father ’ s Name: (First Name) (Middle Name) (Last Name) Address* Pin Code Email ID Annual Income* __________________________________________________________________________________________________________________________________________ Occupation: PROPOSED POLICY DET AILS (Please provide details of your proposed policy) _____________________________________________________________________________________________ (Persons engaged in military service, professional sports, mine workers, fire fighters, water vessel crew , oil field/rig workers, structural workers, window cleaners, junk/and similar hazardous occupation's are excluded under the plan.) T itle* (T ick): Policy Duration 1 Y ear 2 Y ears T elephone Mobile No.: P AN No. Mr . Ms. Mrs. Gender*: Male Female Date of Birth: D D M M Y Y Y Y Single Married Marital Status: Clerical/Administrative Professional – Service/Business Engineer/W orker/Supervisor Driver/Daily W age Labourer T ype: Individual Floater* Proposed Policy Start Date D D M M Y Y Y Y Proposed Policy Start T ime H H : M M Age Band FOR OFFICE USE ONL Y Branch Code : Intermediary Code* : Intermediary Location Code : Intermediary Employee Code : Intermediary Reference Code : Sales Manager Code : Details of POS Aadhar No : or P AN No. : Hospital Daily Cash: Accident Only Accident and Sickness Hospital Cash Accident only Hospital Cash Accident and Sickness 1000 per day - max upto 30 day 18 to 40 41 to 50 51 to 60 61 to 65 66 to 80 375 375 375 375 375 1080 1773 3092 5296 9000 The above sum insured's are only for illustrative purpose. All above mentioned premium is exclusive of GST | Disclaimer: Y our personal accident sum insured can not exceed 10 times of your annual income Others Self Plan Self + Spouse Self + Spouse + 1 Child Self + Spouse + 2 Children Sum Insured ( ` ) 10 Lakhs 20 Lakhs 25 Lakhs 50 Lakhs 75 Lakhs 1 Cr 1.5 Cr 1645 1845 1945 2045 3070 3670 3970 4270 3370 4120 4495 4870 5522 7022 7772 8522 8196 10821 12133 13446 10721 14221 15971 17721 17989 23989 26989 29989 2 Cr 2.5 Cr 15 Lakhs 23726 31726 35726 39726 29463 39463 44463 49463 2769 3219 3444 3669 Figures in ` ILLUSTRA TIVE SUM INSURED FOR PLAN 4 (1 YEAR) IP A Plan - 4 Self Plan Self + Spouse Self + Spouse + 1 Child Self + Spouse + 2 Children Sum Insured ( ` ) 10 Lakhs 20 Lakhs 25 Lakhs 50 Lakhs 75 Lakhs 1 Cr 1.5 Cr 3061 3433 3619 3805 5709 6825 7383 7941 6269 7664 8361 9059 10270 13060 14455 15850 15244 20126 22568 25009 19941 26451 29706 32961 33460 44620 50200 55780 2 Cr 2.5 Cr 15 Lakhs 44131 5901 1 66451 73891 54801 73401 82701 92001 5150 5987 6406 6824 Figures in ` ILLUSTRA TIVE SUM INSURED FOR PLAN 4 (2 YEARS) PROPOSED INSURED(S) INFORMA TION (Please provide more details of the persons who are being covered in this Policy) *Floater Plan: Accidental Death & Permanent disability - Spouse 50%, Children (Max 2) 25% Sr . No. Relationship with Proposer Name Date of Birth (DD/MM/YY) Gender Profession/ Occupation (refer list at the end of the form) Sum Insured Annual Income Name of the Nominee/ Relationship Existing Injury/ Disability (if any) T able of Benefit & Sum Insured T able of Benefit selected (Refer 'T able of Benefit' in the brochure)